")
Chemoembolization (TACE)
Targeted Chemotherapy Delivered Directly to Liver Tumors
Home » Chemoembolization
Fighting Liver Tumors at Their Source
When liver tumors cannot be removed surgically, chemoembolization — also known as TACE (transarterial chemoembolization) — attacks them from the inside. This proven, minimally invasive treatment delivers concentrated chemotherapy medication directly into liver tumors through a small catheter while simultaneously cutting off their blood supply. The result is a powerful one-two punch: high-dose cancer-fighting drugs trapped at the tumor site, combined with starvation of the blood flow tumors need to survive.
Because the chemotherapy is delivered directly to the tumor rather than circulated through your entire body, drug concentrations at the cancer site reach up to 40 times higher than with intravenous chemotherapy — while producing far fewer of the whole-body side effects most people associate with cancer treatment. The procedure takes about 90 minutes, and most patients go home within a day or two.
Chemoembolization has been the standard of care for intermediate-stage liver cancer for over two decades, with landmark clinical trials demonstrating that it significantly extends survival compared to no treatment. It can also serve as a bridge to liver transplant or shrink tumors enough to qualify patients for surgical removal. Dr. Austin Bourgeois performs both TACE and Y90 radioembolization, giving him the expertise to recommend whichever liver-directed therapy offers the best outcome for your specific situation — without the institutional bias that can occur at centers offering only one option.

Hepatocellular Carcinoma (HCC)
The most common form of primary liver cancer and the condition for which TACE has the strongest clinical evidence. International guidelines recommend chemoembolization as the standard first-line treatment for intermediate-stage HCC. In landmark studies, more than 80% of TACE-treated patients were alive at one year, and the procedure achieves visible tumor response in roughly 70% of patients.
Colorectal Cancer Liver Metastases
When colon or rectal cancer spreads to the liver and cannot be surgically removed, chemoembolization using drug-eluting beads loaded with irinotecan (DEBIRI) provides a liver-directed treatment option. Studies show meaningful tumor marker reductions and disease stabilization in the majority of treated patients, often in combination with systemic chemotherapy.
Intrahepatic Cholangiocarcinoma
Bile duct cancers originating within the liver can be difficult to treat when surgery is not feasible. Chemoembolization achieves disease stabilization in over 57% of patients and has enabled some patients to be downstaged to surgical resection. National guidelines include TACE as a treatment option for unresectable intrahepatic cholangiocarcinoma.
Neuroendocrine Tumor Liver Metastases
Carcinoid tumors, pancreatic neuroendocrine tumors, and other NETs that have spread to the liver respond well to chemoembolization, with response rates exceeding 50% even in patients with extensive liver involvement. TACE also provides effective relief from hormonal symptoms such as flushing, diarrhea, and wheezing associated with carcinoid syndrome.
Bridge to Liver Transplant
For patients awaiting liver transplant, TACE is the most commonly used bridging therapy — controlling tumor growth while waiting for a donor organ. Post-transplant survival with TACE bridging reaches 93% at five years. TACE can also downstage tumors that initially exceed transplant size criteria, qualifying patients for potentially curative transplantation.
Tumors Not Responding to Other Treatments
When systemic chemotherapy has stopped working or when patients cannot tolerate whole-body treatment due to side effects, chemoembolization offers a targeted alternative that treats the liver directly while limiting systemic drug exposure.
Understanding the Two Ways TACE Treats Liver Tumors
Chemoembolization works by exploiting a key difference in how healthy liver tissue and liver tumors receive their blood. Your healthy liver gets about 75% of its blood from the portal vein — a large vessel that carries nutrient-rich blood from the digestive system. Liver tumors, however, rely almost entirely on the hepatic artery for their blood supply.
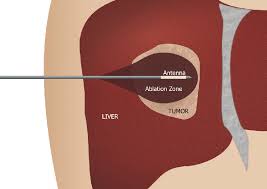
By threading a thin catheter through the hepatic artery directly to the vessels feeding the tumor, your interventional radiologist delivers a concentrated dose of chemotherapy medication precisely where it is needed. Then, tiny particles are injected to physically block those same blood vessels — trapping the chemotherapy drugs inside the tumor and starving it of the oxygen and nutrients it needs to grow.
This dual mechanism is what makes chemoembolization so effective: the tumor receives a massive dose of cancer-fighting medication while simultaneously losing its lifeline. Meanwhile, healthy liver tissue continues to receive blood flow through the portal vein, preserving liver function.
Dr. Bourgeois offers two forms of chemoembolization, each with distinct advantages:
Conventional TACE (cTACE)
In conventional chemoembolization, the chemotherapy medication is mixed with an oily contrast agent called Lipiodol to create a drug-carrying emulsion. This mixture is injected into the tumor’s blood supply, where the oily agent helps the chemotherapy adhere to the tumor tissue. Afterward, tiny absorbable sponge particles are injected to block the feeding arteries. Conventional TACE has the longest track record — over 40 years of clinical use — and the broadest evidence base supporting its effectiveness.
Drug-Eluting Bead TACE (DEB-TACE)
Drug-eluting bead chemoembolization uses specially engineered microscopic beads — roughly the size of grains of sand — that are pre-loaded with chemotherapy medication before the procedure. Once injected into the tumor’s blood supply, these beads accomplish two things simultaneously: they physically block the feeding blood vessels and slowly release the chemotherapy drug over days to weeks, like a time-release capsule embedded directly in the tumor. Clinical studies show that DEB-TACE delivers significantly higher drug concentrations to the tumor with lower levels entering the rest of the body, resulting in less post-procedure pain and fewer systemic side effects than conventional TACE. DEB-TACE is particularly advantageous for patients with more advanced liver disease or who experienced significant side effects from previous conventional TACE sessions.
Which approach is right for you? Both forms of TACE achieve comparable tumor control. Dr. Bourgeois selects the approach best suited to your specific tumor characteristics, liver function, and treatment history. Having expertise in both techniques means your treatment is guided by what works best for you — not by what a particular facility happens to offer.
Who is a Candidate?
Is Chemoembolization Right for You?"
General Eligibility:
The best candidates for chemoembolization typically have adequate liver function (Child-Pugh class A or early B), reasonable overall health and activity level, open main portal vein blood flow, and disease that is confined to or predominantly within the liver. During your consultation, Dr. Bourgeois reviews your imaging, lab work, and complete medical history to determine whether TACE is the optimal approach for your situation — or whether an alternative liver-directed therapy such as Y90 radioembolization may offer a better outcome.
Liver Tumors That Cannot Be Surgically Removed
Patients diagnosed with liver cancer or liver metastases where the number, size, or location of tumors makes surgical resection unsafe or impractical. TACE provides a powerful treatment option when surgery is not on the table, with studies showing it significantly extends survival compared to supportive care alone.
Patients Working Toward Transplant Eligibility
If your tumors currently exceed the size criteria for liver transplant listing, chemoembolization can shrink them enough to qualify — a process called downstaging. Over half of initially ineligible patients treated with TACE achieve successful downstaging, and their long-term post-transplant outcomes are comparable to patients who met criteria from the start.
Patients Seeking a Targeted Alternative to Systemic Chemotherapy
If intravenous chemotherapy has caused intolerable side effects or your tumors have stopped responding to systemic treatment, chemoembolization delivers cancer-fighting drugs directly to the liver while dramatically reducing whole-body exposure. Many patients who struggled with IV chemotherapy tolerate TACE significantly better.
Patients Needing Tumor Control While Awaiting Other Treatments
Whether you are waiting for a transplant donor, preparing for a future surgery, or being evaluated for clinical trials, TACE can keep tumors in check during the waiting period — preventing progression that might disqualify you from those treatments.
What to Expect: Your Chemoembolization Journey
Consultation and Treatment Planning
Dr. Bourgeois reviews your diagnosis, imaging studies, lab results, and complete medical history. He explains how chemoembolization works, discusses whether TACE or another liver-directed therapy is the best fit for your case, and answers your questions. If you have been referred by an oncologist or hepatologist, he coordinates directly with your existing care team to ensure a unified treatment plan. Pre-procedure blood work, including liver and kidney function tests, platelet count, and tumor markers, is obtained. You will receive specific instructions about stopping blood thinners, fasting requirements, and what to bring for your hospital stay.
Procedure Day
You arrive at the hospital, receive an IV line, and are given antibiotics, anti-nausea medication, and pain medication to prepare. Moderate sedation is administered through your IV — you will be relaxed and comfortable but able to communicate throughout the procedure. Through a tiny access point in your groin or wrist, a thin catheter is guided under real-time X-ray imaging through your arterial system to the specific blood vessels feeding your liver tumor. Contrast dye is injected to create a detailed map of the tumor blood supply. A smaller microcatheter — about the diameter of a piece of spaghetti — is then advanced into the precise tumor-feeding arteries, and the chemotherapy-carrying agents are carefully delivered until the target vessels are blocked. A final set of images confirms successful treatment. The catheter is removed, and pressure is applied to the access site — no stitches are needed. The entire procedure typically takes 60 to 90 minutes.
Hospital Recovery
Following the procedure, you rest in bed for four to six hours with monitoring of vital signs, pain levels, and the catheter access site. IV fluids, pain medication, and anti-nausea medication are provided as needed. Most patients stay overnight for one to two nights, though some DEB-TACE patients may go home the same day. Post-embolization syndrome — a combination of abdominal discomfort, fatigue, nausea, and sometimes low-grade fever — is common during the first 24 to 72 hours and is managed with medication in the hospital. You are discharged once your pain is well-controlled with oral medication, you are eating and drinking, and your vital signs are stable.
Recovery at Home and Follow-Up
You go home with prescriptions for pain medication, anti-nausea medication, and a stomach protector. Most patients feel noticeably better each day, with the worst of post-embolization symptoms resolving within the first week. Fatigue and reduced appetite may linger for two to three weeks. Most patients resume light daily activities and desk work within one week and are back to their full routine by four to six weeks. Follow-up blood work is drawn at approximately three weeks to check liver function, and your first follow-up imaging scan — typically a contrast-enhanced CT or MRI — occurs at four to six weeks to assess how the tumor responded to treatment.
How Many Treatments Will I Need?
Most patients require two to three chemoembolization sessions, spaced four to eight weeks apart. Treatment is performed “on demand” — meaning additional sessions are scheduled only when follow-up imaging shows they are needed, rather than on a fixed schedule. Some patients achieve excellent tumor control with a single session; others benefit from periodic retreatment over months or years. Dr. Bourgeois discusses a personalized treatment plan during your consultation.
Why Patients Choose TACE






TACE vs. Other Liver Cancer Treatments
Choosing the right treatment depends on your diagnosis, tumor characteristics, liver function, and overall health. Here is how chemoembolization compares to other common approaches for liver tumors:
Chemoembolization (TACE) vs. Y90 Radioembolization
Chemoembolization (TACE) vs. Y90 Radioembolization
Both are catheter-based, liver-directed treatments performed by an interventional radiologist, but they work through fundamentally different mechanisms. TACE delivers chemotherapy plus blood vessel blockage. Y90 delivers internal radiation via microscopic beads. Dr. Bourgeois performs both procedures and can recommend the approach best suited to your situation.
- TACE is generally preferred for smaller, well-defined tumors in patients with good liver function, and when cost per session is a consideration. Y90 is often preferred for larger or more diffuse tumors, bilobar disease, and patients with portal vein tumor invasion.
- Y90 is typically performed as an outpatient procedure, while TACE usually requires an overnight hospital stay.
- Y90 typically requires one to two sessions; TACE averages two to three sessions over the course of treatment.
- Y90 demonstrated significantly longer time before tumor progression in head-to-head studies — more than 26 months compared to roughly 7 months with TACE.
- Both treatments produce comparable overall survival in meta-analyses. The best choice depends on individual patient factors, which Dr. Bourgeois evaluates during your consultation.
- Internal link: Learn more about Y90 Radioembolization → /y90-radioembolization-huntsville
TACE vs. Intravenous (Systemic) Chemotherapy
Systemic chemotherapy and newer immunotherapy/targeted therapy drugs circulate throughout your entire body. TACE concentrates treatment at the liver.
- TACE delivers drug concentrations at the tumor up to 40 times higher than systemic therapy can achieve, while dramatically reducing whole-body drug exposure.
- Patients undergoing TACE experience significantly less hair loss, nausea, immune suppression, and nerve damage compared to intravenous chemotherapy.
- TACE and systemic therapy are increasingly used together — landmark 2024 and 2025 clinical trials show that combining TACE with immunotherapy nearly doubles progression-free survival compared to TACE alone.
- Systemic therapy can treat cancer throughout the body, including metastases outside the liver. TACE treats only liver tumors. When disease exists both inside and outside the liver, your oncologist and Dr. Bourgeois may recommend a combined approach.
TACE vs. Surgical Resection
Surgery remains the gold standard when liver tumors can be safely and completely removed. TACE plays a complementary role:
- TACE is the treatment of choice when tumors cannot be surgically removed due to their size, number, location, or insufficient remaining healthy liver.
- Chemoembolization can shrink tumors to make previously inoperable patients candidates for surgical removal.
- TACE is less invasive than surgery, with shorter recovery and lower immediate risk — making it appropriate for patients whose overall health may not tolerate a major operation.
- For patients waiting for liver transplant, TACE controls tumor growth during the wait and can downstage tumors to meet transplant eligibility requirements.
Your Recovery Timeline After Chemoembolization
We believe in preparing patients honestly. While chemoembolization is well-tolerated compared to systemic chemotherapy, the first few days after treatment are genuinely challenging for most patients. Knowing what to expect helps you plan ahead and worry less when normal post-procedure symptoms appear.
Understanding the Investment in Your Treatment
We believe in transparency about treatment costs because financial uncertainty should not compound the stress of a cancer diagnosis.
Chemoembolization is a specialized hospital-based procedure. Total costs per session — including the hospital stay, medications, imaging, facility fees, and physician services — typically range from $18,000 to $25,000 before insurance. Most patients require two to three sessions over the course of their treatment.
The good news: chemoembolization is broadly covered by insurance when medically indicated. Blue Cross Blue Shield of Alabama, Medicare, Medicaid, TRICARE, UnitedHealthcare, Aetna, and Cigna all cover TACE for standard indications including unresectable liver cancer, bridge to transplant, and liver metastases. Prior authorization is typically required, and our team handles this process on your behalf.
For Medicare patients, Part B covers 80% of the approved amount after your annual deductible. Medigap supplemental plans often cover the remaining 20% coinsurance. Average Medicare out-of-pocket costs for chemotherapy procedures run approximately $250 per visit.
Veterans receiving care through the VA system may be eligible for community care authorization to receive TACE locally in Huntsville rather than traveling to the Birmingham VA Medical Center. Our office can assist with the referral and authorization process for VA patients.
Before each procedure, our team verifies your insurance coverage, obtains necessary authorizations, and provides you with a clear estimate of expected out-of-pocket costs so you can plan accordingly.



What Happens If Chemoembolization Stops Working?
This is one of the most common questions patients ask — and one that very few medical websites address directly. We think it deserves a straightforward answer.
Chemoembolization does not work indefinitely for all patients. Some tumors stop responding after multiple sessions, and new lesions may develop over time. Current clinical guidelines suggest that if there is insufficient tumor response after two to three well-performed TACE sessions, it is time to consider alternative or additional treatments. This is not a failure — it is the natural course of managing a complex disease.
If TACE is no longer the best option, several evidence-based pathways are available:
Y90 Radioembolization: Uses a completely different mechanism — targeted radiation rather than chemotherapy — and may be effective in tumors that have stopped responding to TACE. Dr. Bourgeois offers both treatments in Huntsville, so transitioning does not require a new physician or a different facility.
Systemic Immunotherapy or Targeted Therapy: Newer drugs including atezolizumab, bevacizumab, lenvatinib, and pembrolizumab have transformed outcomes for advanced liver cancer. Your oncologist may recommend systemic treatment either alone or in combination with continued liver-directed therapy.
Liver Transplant Evaluation: If your tumor burden is within or near transplant criteria, TACE treatment may have already positioned you for transplant candidacy. Referral to a transplant center for evaluation is a critical step.
Thermal Ablation: For smaller remaining tumors, microwave or radiofrequency ablation may provide targeted destruction through heat. Dr. Bourgeois also performs microwave ablation and can determine whether it is appropriate for your situation.
Clinical Trials: New treatments are constantly being studied. Dr. Bourgeois can help identify clinical trial options through the regional oncology network.
The key message: running out of options with one treatment does not mean running out of options entirely. Dr. Bourgeois coordinates closely with your oncologist, hepatologist, and transplant team to ensure there is always a clear next step in your care plan.

Expert Liver-Directed Therapy — Close to Home
Dr. Austin Bourgeois brings academic-caliber liver-directed therapy expertise to Huntsville. His credentials include:
- Board-certified in both Diagnostic Radiology and Interventional Radiology & Diagnostic Radiology
- Fellowship-trained in Vascular and Interventional Radiology at the Medical University of South Carolina — one of the nation’s premier IR training programs — with advanced training in embolization therapy
- Published researcher in interventional oncology with peer-reviewed manuscripts on radioembolization dosimetry, imaging verification, and procedural techniques in the Journal of Vascular and Interventional Radiology (JVIR)
- Member of the JVIR editorial board
- Performs BOTH chemoembolization and Y90 radioembolization — giving him the expertise to recommend whichever treatment offers you the best outcome, without institutional bias toward a single modality
- Boston Scientific TheraSphere Advanced User, indicating proctor-level expertise in liver-directed therapies
- Practicing in North Alabama since 2016 with deep relationships across the regional oncology and gastroenterology referral network
What this means for you: your chemoembolization is performed by a physician who has not only extensive procedural experience but also published research on optimizing liver-directed therapy outcomes. You receive the same quality of care available at major academic medical centers — with the convenience of staying close to home, your family, and your support system.
Dr. Bourgeois works closely with your oncologist, hepatologist, and any transplant team involved in your care. Whether you have been referred by Clearview Cancer Institute, your gastroenterologist, or are seeking a second opinion, we welcome the opportunity to review your case and discuss your treatment options.
Frequently Asked Questions
Quick answers about chemoembolization (TACE) — what to expect, recovery, and results.
Chemoembolization, also called TACE (transarterial chemoembolization), is a minimally invasive procedure that delivers concentrated chemotherapy medication directly into liver tumors through a catheter placed in the hepatic artery while simultaneously blocking the blood vessels feeding the tumor. This traps high-dose cancer-fighting drugs at the tumor site while cutting off its blood supply. The procedure is performed by an interventional radiologist — a physician who specializes in image-guided, catheter-based treatments.
Chemoembolization achieves tumor response — meaning visible shrinkage or growth arrest — in approximately 70% of treated patients. In landmark clinical trials, more than 80% of TACE patients were alive at one year, compared to 63% with supportive care alone. Well-selected intermediate-stage liver cancer patients achieve median survival of two to three years, with some patients surviving significantly longer. Effectiveness varies by cancer type, stage, liver function, and individual tumor biology.
Conventional TACE mixes chemotherapy with an oily carrier agent (Lipiodol), followed by embolization with sponge particles. Drug-eluting bead TACE uses pre-loaded microspheres that simultaneously block blood vessels and slowly release chemotherapy over days. Both achieve similar tumor control, but DEB-TACE generally causes less post-procedure pain and fewer systemic side effects. Dr. Bourgeois performs both techniques and selects the approach best suited to your individual case.
TACE delivers chemotherapy plus blood vessel blockage, while Y90 delivers targeted radiation via microscopic beads. Y90 is typically outpatient with fewer sessions needed, while TACE usually requires an overnight stay and averages more sessions. Y90 shows longer time to tumor progression in comparative studies and can treat patients with portal vein tumor invasion, where TACE is generally not recommended. Dr. Bourgeois performs both procedures and can recommend the best option based on your specific diagnosis and tumor characteristics.
During the procedure itself, moderate sedation keeps you comfortable — most patients feel pressure but not significant pain. After the procedure, abdominal pain, cramping, and discomfort are common for the first one to three days as part of post-embolization syndrome. We manage this with strong pain medication in the hospital and oral medications at home. We want to be transparent: some patients describe the first 48 hours as quite uncomfortable, while others experience only mild discomfort. Pain medication is available proactively — there is no need to tough it out.
Most patients go home after one to two nights in the hospital. Post-embolization syndrome — pain, nausea, fatigue, and low-grade fever — typically peaks in the first two to three days and resolves within a week. Most patients resume light activities and desk work within one to two weeks. Full recovery to baseline energy levels takes four to six weeks. DEB-TACE patients generally experience a faster recovery with less intense symptoms.
Most patients require two to three sessions spaced four to eight weeks apart. Treatment is scheduled based on your imaging response — additional sessions occur only when follow-up scans show they would be beneficial, not on a fixed schedule. Some patients achieve excellent results with one session, while others may receive periodic treatments over a longer time period.
Yes. Chemoembolization is covered by virtually all major insurance plans when medically indicated, including Blue Cross Blue Shield of Alabama, Medicare, TRICARE, UnitedHealthcare, Aetna, and Cigna. Prior authorization is required, and our team manages this entire process for you. We provide a clear estimate of any expected out-of-pocket costs before your procedure.
Most patients experience minimal hair thinning — far less than with traditional intravenous chemotherapy. Because the chemotherapy is delivered directly to the liver tumor rather than circulated throughout the body, the whole-body drug levels are dramatically lower. Significant hair loss is uncommon, and when it occurs, it is typically mild enough that others do not notice.
Yes. Chemoembolization is the most commonly used therapy to bridge patients to liver transplant and to downstage tumors that initially exceed transplant criteria. Over half of patients treated with TACE for downstaging achieve successful transplant eligibility, and their long-term post-transplant outcomes are excellent — with five-year survival reaching 93% in well-selected patients.
If TACE is no longer producing adequate tumor response, several next-step options exist: Y90 radioembolization (which uses a completely different mechanism), systemic immunotherapy or targeted therapy, thermal ablation for smaller tumors, liver transplant evaluation, or clinical trial enrollment. Dr. Bourgeois coordinates with your oncology team to ensure there is always a clear path forward. Running out of options with one treatment does not mean running out of options entirely.
TACE may not be appropriate for patients with severely compromised liver function (advanced cirrhosis, Child-Pugh class C), complete blockage of the main portal vein, cancer that has spread extensively outside the liver, severe kidney impairment, active untreated infection, or significant blood clotting disorders. These factors are carefully evaluated before any treatment decision is made.
Have more questions? Dr. Bourgeois is happy to discuss your specific situation.
Schedule Your Consultation