")
Kidney Cryoablation
Destroy Small Kidney Tumors by Freezing — Without Surgery, Without Losing Your Kidney
Home » Kidney Cryoablation
You Were Told You Have a Kidney Mass — Here Is What You Need to Know
If you are reading this, chances are a CT scan or MRI revealed something unexpected on your kidney — and the words “mass” or “tumor” sent your mind racing. Take a breath. You are in the right place, and the news may be better than you think.
Most small kidney masses are found incidentally — during imaging ordered for something else entirely, like back pain or a routine check-up. This is increasingly common as imaging technology improves, and it means these masses are being caught earlier and at smaller sizes than ever before. Up to 30 percent of small kidney masses turn out to be benign (not cancer) when biopsied. And for the ones that are cancerous, small kidney tumors caught at this stage are among the most treatable cancers in all of medicine.
Kidney cryoablation is a minimally invasive treatment that destroys small kidney tumors by freezing them to lethal temperatures through a needle-thin probe inserted through the skin. There are no surgical incisions, no kidney removal, and no stitches. The tumor is destroyed in place, and your kidney continues to function normally.
This is not a compromise or a second-choice treatment. A landmark Johns Hopkins study following patients for ten years found that cryoablation achieves 94 percent disease-specific survival — identical at five and ten years — matching the outcomes of surgical removal for small kidney tumors. And cryoablation does it with dramatically less risk: fewer than 3 percent of patients experience major complications compared to 15 to 20 percent with surgery, and 95 percent of cryoablation patients maintain normal kidney function at three years compared to just 70 percent after partial nephrectomy.
The procedure typically takes one to three hours, most patients go home the same day or the next morning, and the majority return to their normal routine within one to two weeks. Compare that to partial nephrectomy, which typically requires a three-to-five-day hospital stay and four to six weeks of recovery.
Dr. Austin Bourgeois performs percutaneous kidney cryoablation using real-time CT guidance — the most precise, least invasive approach available. As a board-certified interventional radiologist, he specializes in image-guided treatments that eliminate tumors while preserving healthy tissue and organ function.

Kidney Conditions We Treat with Cryoablation
Small Renal Cell Carcinoma (Stage T1a)
The most common indication for kidney cryoablation. Stage T1a tumors — those four centimeters or smaller confined to the kidney — are ideal candidates for cryoablation, with technical success rates of 94 to 100 percent for tumors under three centimeters. International guidelines from the American Urological Association, the National Comprehensive Cancer Network, and the European Association of Urology all endorse thermal ablation as an appropriate treatment for T1a renal masses, particularly in patients with comorbidities, advanced age, or impaired kidney function.
Incidentally Discovered Kidney Masses
The majority of small kidney tumors today are found unexpectedly during imaging performed for unrelated reasons. If your CT scan or MRI revealed a small kidney mass and you are researching your options, cryoablation offers a way to definitively treat the mass with minimal disruption to your life. A biopsy is typically performed at the beginning of the cryoablation procedure to confirm the diagnosis — and if the mass turns out to be benign (which occurs in 20 to 30 percent of cases), that information guides ongoing management.
Tumors in Patients with a Single Kidney
Preserving kidney function is paramount when you have only one functioning kidney — whether due to previous surgery, congenital absence, or a non-functioning opposite kidney. Cryoablation destroys only the tumor and a small surrounding margin, leaving the maximum amount of healthy kidney tissue intact. Studies show that 95 percent of cryoablation patients remain free of chronic kidney disease at three years, compared to just 70 percent after partial nephrectomy.
Bilateral Kidney Tumors
When tumors develop in both kidneys simultaneously, cryoablation can treat masses on both sides while preserving the maximum amount of functional kidney tissue on each side. This is especially important for patients with hereditary conditions like Von Hippel-Lindau disease who may develop multiple kidney tumors throughout their lifetime and need to preserve as much kidney function as possible for future treatments.
Tumors in Patients with Significant Health Conditions
Patients with heart disease, lung disease, diabetes, obesity, or other conditions that increase the risk of general anesthesia and major surgery are often excellent candidates for cryoablation. The procedure can be performed under conscious sedation in some cases, involves minimal blood loss, and allows same-day or next-day discharge — dramatically reducing the physiological stress compared to surgical approaches.
Hereditary Kidney Cancer Syndromes
Patients with Von Hippel-Lindau disease, hereditary papillary renal cell carcinoma, Birt-Hogg-Dubé syndrome, and other genetic conditions that predispose to multiple kidney tumors over a lifetime benefit enormously from cryoablation’s tissue-sparing and repeatable nature. Rather than removing sections of kidney with each new tumor, cryoablation can be performed multiple times while preserving long-term kidney function.
Destroying Tumors by Freezing — From the Inside Out
Cryoablation uses extreme cold to destroy cancer cells — the opposite approach from heat-based ablation techniques, but with a unique advantage: the treatment zone is visible in real time on CT imaging as a ball of ice that forms around the tumor.
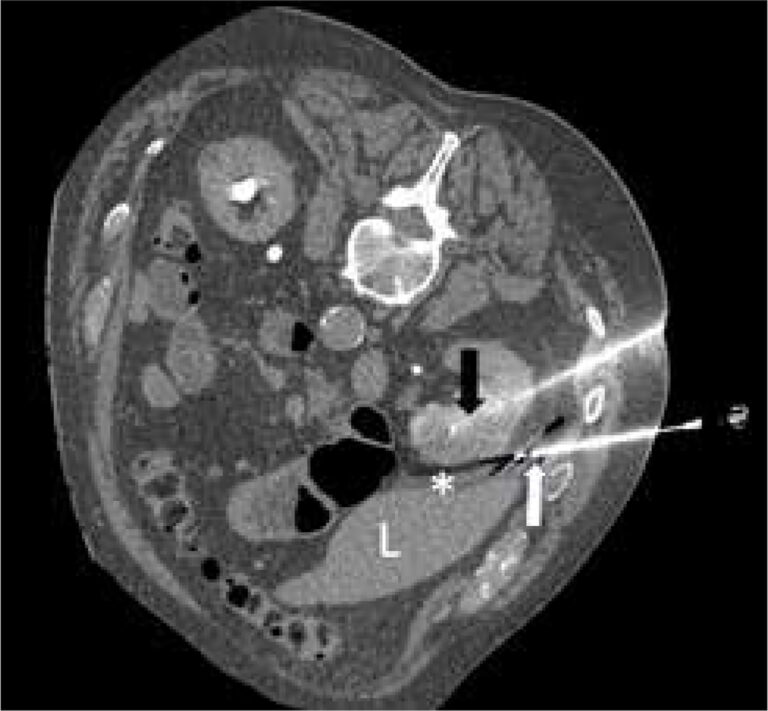
A thin needle-like probe called a cryoprobe — roughly the diameter of a pencil lead — is guided through the skin and into the center of the kidney tumor using real-time CT imaging. When activated, compressed argon gas flows through the probe and rapidly expands at the tip, dropping temperatures to approximately negative 160 degrees Celsius (negative 256 degrees Fahrenheit). This creates a growing sphere of ice — called an ice ball — that engulfs the tumor and a surrounding margin of tissue.
Cell death occurs through multiple mechanisms. As tissue freezes, ice crystals form inside the cancer cells, physically rupturing their membranes. Simultaneously, the spaces between cells become hyper-concentrated with salt as water freezes out of solution, drawing remaining liquid out of cells through osmotic shock. The freezing also destroys the tiny blood vessels feeding the tumor, cutting off its blood supply through microvascular thrombosis. The result is complete, irreversible destruction of the frozen tissue.
The standard protocol uses a double freeze-thaw cycle: a ten-minute freeze, followed by a five-to-eight-minute passive thaw, then a second ten-minute freeze. The second freeze is actually more lethal than the first because previously frozen tissue has roughly four times greater thermal conductivity — meaning the ice penetrates faster and reaches more extreme temperatures during the second cycle.
During the procedure, the growing ice ball is clearly visible on CT imaging as a dark, well-defined sphere. Dr. Bourgeois monitors this in real time, ensuring the ice ball extends five to ten millimeters beyond the visible tumor edge in all directions. This safety margin — where temperatures reach the lethal zone of negative 20 to negative 40 degrees Celsius — is critical for destroying any microscopic cancer cells at the tumor periphery. The ability to see the treatment zone forming in real time is a significant advantage of cryoablation over heat-based techniques, where the ablation zone boundary is less precisely visualized.
Over the following weeks and months, the destroyed tissue is gradually absorbed by the body. On follow-up imaging, the treated area shrinks progressively — approximately 26 percent at three months, 56 percent at one year, and 75 percent at three years — eventually resolving into a small scar or area of fat replacement.
Why Cryoablation Instead of Radiofrequency or Microwave Ablation for Kidney Tumors?
If you have researched kidney tumor ablation, you may have encountered references to radiofrequency ablation (RFA) or microwave ablation (MWA) — heat-based techniques that are widely used for liver tumors. While all three technologies can destroy kidney tumors, cryoablation has emerged as the preferred ablation method for kidney masses for several important reasons:
Cryoablation produces significantly fewer retreatments than radiofrequency ablation — 1.3 percent versus 8.5 percent in comparative studies — and lower rates of tumor progression (5.2 percent versus 12.9 percent). The visible ice ball allows real-time monitoring of the treatment zone, providing immediate confirmation that the entire tumor has been covered with adequate margins. Cryoablation is also less painful than heat-based techniques, as freezing has a natural anesthetic effect on nerve endings. And for tumors located near the ureter or renal collecting system, cryoablation is safer because it causes less damage to these structures than heat-based approaches.
For these reasons, percutaneous cryoablation is the dominant ablation technique used for kidney tumors at major academic medical centers, and it is the approach Dr. Bourgeois uses for renal mass ablation.


Who is a Candidate?
Is Kidney Cryoablation Right for You?
The best candidates for kidney cryoablation typically have tumors four centimeters or smaller (ideally three centimeters or smaller for the highest success rates), a tumor location accessible by the percutaneous (through-the-skin) approach, no cancer spread beyond the kidney, and no active urinary tract infection or uncorrectable blood clotting disorder. During your consultation, Dr. Bourgeois reviews your imaging, lab work, and medical history to determine whether cryoablation is the optimal approach for your specific tumor — or whether surgical referral or active surveillance would better serve your situation.
Small Kidney Tumors (T1a — 4cm or Smaller)
The strongest candidates for cryoablation have tumors four centimeters or smaller confined to the kidney. Tumors three centimeters or smaller achieve the highest success rates — 97 to 100 percent complete ablation — with outcomes that match surgical removal. Tumors in the three-to-four centimeter range are also treatable with excellent results, typically requiring additional cryoprobes to ensure complete coverage. Tumor location matters as well: exophytic tumors (those that protrude outward from the kidney surface) and posterior tumors are particularly well-suited for the percutaneous approach.
Patients Who Want to Preserve Kidney Function
Even when surgery is technically possible, some patients and their physicians choose cryoablation because of its superior kidney-function preservation. At three years, 95 percent of cryoablation patients remain free of chronic kidney disease, compared to just 70 percent after partial nephrectomy. This advantage is meaningful for all patients but especially important for those with borderline kidney function, diabetes, hypertension, or a single functioning kidney.
Patients with Health Conditions That Increase Surgical Risk
Heart disease, lung disease, obesity, diabetes, advanced age, and blood-thinning medications that cannot be safely stopped all increase the risk of complications from surgery. Cryoablation offers these patients a treatment option with a major complication rate under 3 percent — compared to 15 to 20 percent for partial nephrectomy. The procedure involves minimal blood loss and can be performed under conscious sedation when general anesthesia poses too great a risk.
Patients Choosing Cryoablation as a First-Line Option
Cryoablation is not only for patients who cannot have surgery. Guideline-supported clinical evidence shows equivalent cancer-specific survival for small kidney tumors, and an increasing number of informed patients are proactively choosing cryoablation for its dramatically shorter recovery, superior kidney preservation, lower complication rate, and equivalent cancer control. If you have been told surgery is your only option for a small kidney tumor, it is worth exploring whether cryoablation could achieve the same outcome with less impact on your body and your life.
What to Expect: Your Kidney Cryoablation Journey
Consultation and Treatment Planning
Dr. Bourgeois reviews your diagnosis, imaging studies (CT or MRI), lab results, and complete medical history. He examines the tumor size, location, and relationship to surrounding structures like the ureter, renal collecting system, and nearby organs. He explains how cryoablation works, discusses whether your tumor characteristics make you a strong candidate, and compares cryoablation to surgical options and active surveillance. If you have been referred by a urologist or oncologist, he coordinates directly with your care team. Pre-procedure blood work — including kidney function (creatinine and GFR), coagulation studies, and a complete blood count — is obtained. You receive specific instructions about stopping blood thinners, fasting requirements, and what to expect on procedure day.
Procedure Day
You arrive at the hospital and check in at the day surgery unit. An IV is placed, monitoring equipment is attached, and you change into a hospital gown. For most kidney cryoablations, general anesthesia is used — you will be completely asleep and feel nothing. Once under anesthesia, the interventional radiology team positions you face-down (prone) or at a slight angle in the CT scanner. Using CT imaging for precise guidance, Dr. Bourgeois makes a small skin puncture and advances the thin cryoprobe through the back muscles and into the center of the kidney tumor. For tumors under two centimeters, one to two probes are typically sufficient. Tumors between two and three centimeters may require two to three probes, and larger tumors may need four or more probes arranged to ensure the ice ball completely covers the tumor with adequate margins. A biopsy of the tumor is typically performed at this point to confirm the diagnosis. The cryoablation system is then activated for the first ten-minute freeze cycle. CT scans are obtained every few minutes to monitor the growing ice ball and confirm it is extending beyond the tumor edge. After a five-to-eight-minute passive thaw, the second ten-minute freeze cycle is performed. If the tumor is located near the ureter or bowel, Dr. Bourgeois may use hydrodissection — injecting sterile fluid to push vulnerable structures away from the freezing zone — or pyeloperfusion — running warm saline through the collecting system to protect it from freezing injury. After the final thaw, the probes are removed and a small bandage is applied. No stitches are needed. The entire procedure typically takes one to three hours.
Recovery and Discharge
You wake up in the recovery area and are monitored for several hours. Vital signs, pain levels, and the small puncture sites are checked regularly. Pain after kidney cryoablation is typically very mild — studies report average pain scores of 1.8 out of 10 on the first day. Many patients describe feeling as though they did nothing more than a routine medical visit. Blood work is checked to confirm kidney function is stable. Once you are eating, drinking, and comfortable, you are cleared for discharge. Most patients go home the same day — within four to six hours of the procedure. Some patients, particularly those with larger tumors or complex cases, may stay overnight for observation.
Recovery at Home and Follow-Up
You go home with instructions to rest for the first day or two, keep the puncture sites clean and dry, and avoid heavy lifting for approximately one week. Most patients return to light daily activities and desk work within two to three days. Many patients require only over-the-counter pain medication, and some need none at all. Full return to normal activities, including exercise, typically occurs within one to two weeks — a fraction of the four-to-six-week recovery after partial nephrectomy. Your first follow-up imaging scan — a contrast-enhanced CT or MRI — is performed at approximately one month to confirm complete tumor destruction. Success appears as an area with no contrast enhancement (no blood flow) that is slightly larger than the original tumor. After that, imaging is repeated at three months, six months, twelve months, and then annually for at least five years. On each scan, the treated area gradually shrinks — a normal and expected finding that confirms the ablated tissue is being absorbed.
What If the Biopsy Shows a Benign Mass?
Approximately 20 to 30 percent of small kidney masses biopsied during cryoablation turn out to be benign — not cancer. If this is the case, the cryoablation still treats the mass definitively, eliminating the need for ongoing surveillance imaging and the anxiety of watching and waiting. Some patients and their physicians may choose to abort the ablation if the biopsy result is available quickly and shows a clearly benign diagnosis, but in most cases, treating the mass provides peace of mind and avoids years of follow-up imaging for an indeterminate lesion.
Why Patients Choose Cryoablation







Cryoablation vs. Other Kidney Tumor Treatments
Choosing the right treatment for a small kidney tumor depends on tumor size, location, your overall health, and your kidney function. Here is how cryoablation compares to the other common approaches — and how Dr. Bourgeois helps you navigate the decision:
Cryoablation vs. Partial Nephrectomy (Kidney-Sparing Surgery)
- Cancer-specific survival is comparable. A meta-analysis of over 6,400 patients found no significant difference in overall survival or cancer-specific survival between cryoablation and partial nephrectomy for T1a tumors. The Johns Hopkins 10-year study confirmed 94 percent disease-specific survival with cryoablation.
- Cryoablation has dramatically fewer complications: major complication rates of approximately 3 percent versus 15 to 20 percent for partial nephrectomy. Average blood loss with cryoablation is under 15 milliliters versus over 100 milliliters with surgery.
- Kidney function preservation is significantly better with cryoablation. At three years, 95 percent of cryoablation patients are free of chronic kidney disease versus 70 percent after partial nephrectomy. This translates to better long-term cardiovascular health and fewer restrictions on future medications.
- Recovery is dramatically faster: same-day discharge versus three-to-five-day hospital stay. Return to normal activities in one to two weeks versus four to six weeks.
- Cryoablation does have a higher rate of local recurrence (approximately 5 to 10 percent versus 1 to 3 percent for surgery). However, recurrences detected on surveillance imaging can be retreated with a second cryoablation — and cancer-specific survival remains equivalent.
- Surgery may be preferred for tumors larger than four centimeters, tumors with complex anatomy involving the renal hilum, or when a tissue diagnosis requiring the entire tumor is needed.
Cryoablation vs. Radical Nephrectomy (Complete Kidney Removal)
- Radical nephrectomy — removing the entire kidney — is generally considered overtreatment for small kidney tumors that can be treated with nephron-sparing approaches. Both partial nephrectomy and cryoablation preserve kidney function and achieve equivalent cancer control for T1a tumors.
- If you have been told you need your entire kidney removed for a small tumor (under four centimeters), seeking a second opinion is reasonable. Guideline organizations recommend nephron-sparing approaches whenever feasible for small renal masses.
- Cryoablation preserves the most kidney tissue of any treatment approach — an advantage that becomes increasingly important with age, as kidney function naturally declines over time.
Cryoablation vs. Active Surveillance (Watchful Waiting)
- Active surveillance — monitoring the tumor with regular imaging without immediate treatment — is an appropriate option for some patients, particularly those over 75 or with serious competing health conditions where the tumor is unlikely to affect their life expectancy.
- However, active surveillance carries the psychological burden of living with a known tumor and the risk that the tumor may grow beyond the ideal treatment window. Approximately one-third of surveilled tumors grow enough to eventually require intervention.
- For patients who are healthy enough for treatment and prefer definitive action, cryoablation offers a way to resolve the uncertainty with minimal risk and rapid recovery — while the tumor is still at its most treatable size.
- Bourgeois discusses both cryoablation and active surveillance during your consultation and helps you understand which approach best fits your specific medical situation, life expectancy, and personal preferences.
Your Recovery Timeline After Kidney Cryoablation
One of the most consistent things patients say after kidney cryoablation is that recovery was far easier than they expected. Many describe it as feeling like they had gone for a routine medical visit rather than a cancer treatment. Here is an honest timeline so you know exactly what to anticipate.
Understanding the Investment in Your Treatment
We believe in financial transparency because worrying about costs should not add to the stress of a kidney mass diagnosis.
Kidney cryoablation is covered by all major insurance plans when medically indicated, including Blue Cross Blue Shield of Alabama, Medicare, Medicaid, TRICARE, UnitedHealthcare, Aetna, and Cigna. The procedure is billed under CPT code 50593 (percutaneous renal cryoablation). Prior authorization is typically required, and our team handles this process on your behalf.
For Medicare patients, the hospital outpatient facility fee for kidney cryoablation is approximately $10,400, with Medicare Part B covering 80 percent of the approved amount after your annual deductible. Medigap supplemental plans often cover the remaining 20 percent coinsurance. Your total out-of-pocket cost depends on your specific plan but is generally a fraction of the total procedure cost.
Kidney cryoablation is significantly less expensive than partial nephrectomy when total costs are considered — including shorter hospital stays (same-day versus three to five days), faster return to work (days versus weeks), and fewer complications requiring additional treatment.
Veterans receiving care through the VA system may be eligible for community care authorization to receive kidney cryoablation locally in Huntsville rather than traveling to the Birmingham VA Medical Center. Military families covered by TRICARE are also covered for the procedure when medically indicated. Our office can assist with the referral and authorization process.
Before your procedure, our team verifies your insurance coverage, obtains necessary authorizations, and provides you with a clear estimate of expected out-of-pocket costs so you can plan accordingly.


Honest Answers About the Limits of Cryoablation
Not every kidney tumor is best treated with cryoablation — and we believe in being upfront about that from the start. Here are the situations where Dr. Bourgeois may recommend a different approach, and what your options look like:
Tumors Larger Than 4 Centimeters: While cryoablation can technically treat tumors up to seven centimeters, success rates decline for tumors above four centimeters, and the risk of incomplete treatment increases. For tumors in the four-to-seven centimeter range, partial nephrectomy generally offers better local control. Dr. Bourgeois will be transparent about where cryoablation reaches its limits and refer you to a urologic surgeon when surgery offers a meaningfully better outcome.
Tumors Invading the Renal Vein or Collecting System: Tumors that have grown into the main renal vein or extensively involve the central collecting system of the kidney are generally not appropriate for cryoablation. These tumors require surgical management to achieve complete removal. Imaging performed during your consultation helps identify these features.
When a Full Tissue Specimen Is Needed: In rare cases, a complete pathological analysis of the entire tumor is necessary for diagnosis or staging. Since cryoablation destroys the tumor in place, only a biopsy specimen is available. If your medical team determines that a full surgical specimen is essential, partial nephrectomy would be recommended.
Active Surveillance as an Alternative: For some patients — particularly those over 75, those with serious competing health conditions, or those with very small (under one centimeter) tumors that may be benign — active surveillance with regular imaging may be the most appropriate initial strategy. Dr. Bourgeois discusses this option openly and supports patients who choose surveillance, while ensuring they understand when intervention would become recommended.
What If Cryoablation Leaves Residual Tumor?: In approximately 5 to 10 percent of cases, follow-up imaging may show a small area of residual or recurrent tumor. This is not a treatment failure in the traditional sense — it is detected early through the structured surveillance program and is almost always treatable with a repeat cryoablation session. The ability to retreat safely is one of cryoablation’s built-in advantages. Cancer-specific survival remains equivalent to surgery even accounting for this retreatment rate.

Expert Kidney Tumor Treatment — Close to Home
If you have been diagnosed with a small kidney tumor in North Alabama, you may have been told your options are surgery or active surveillance. What many patients are not told — and what many urologists do not mention during the initial consultation — is that percutaneous cryoablation performed by an interventional radiologist is a guideline-endorsed treatment option with outcomes matching surgery for small tumors.
This referral gap is common nationwide. Patients who discover cryoablation often do so through their own research, a second opinion, or a physician who specifically recommends interventional radiology evaluation.
Dr. Austin Bourgeois brings this capability to Huntsville. His credentials include:
- Board-certified in both Diagnostic Radiology and Interventional Radiology & Diagnostic Radiology
- Fellowship-trained in Vascular and Interventional Radiology at the Medical University of South Carolina — one of the nation’s premier IR training programs — with specialized training in image-guided tumor ablation
- Published researcher in interventional oncology with peer-reviewed manuscripts in the Journal of Vascular and Interventional Radiology (JVIR)
- Member of the JVIR editorial board
- Expertise in CT-guided percutaneous ablation — the most precise, least invasive approach for kidney tumor treatment
- Also performs the full spectrum of liver-directed therapies (microwave ablation, chemoembolization, Y90 radioembolization), demonstrating broad interventional oncology expertise
- Practicing in North Alabama since 2016 with established relationships across the regional urology, oncology, and primary care referral network
What this means for you: your kidney cryoablation is performed by a fellowship-trained interventional radiologist with published research in interventional oncology, editorial-board-level involvement in the specialty’s leading journal, and the image-guided expertise that is the foundation of precise, safe tumor ablation. You receive the same quality of care available at UAB or Vanderbilt — with the convenience of staying in Huntsville, close to your family, your urologist, and your support system.
Whether you have been referred by your urologist, are seeking a second opinion, or discovered cryoablation through your own research and want to explore it as an option, Dr. Bourgeois welcomes the opportunity to review your case and discuss your options honestly.
Frequently Asked Questions
Quick answers about kidney cryoablation — effectiveness, recovery, and what to expect.
For tumors four centimeters or smaller (T1a), yes. A Johns Hopkins study following patients for ten years found 94 percent disease-specific survival with cryoablation — identical at five and ten years. A meta-analysis of over 6,400 patients found no significant difference in overall survival or cancer-specific survival between cryoablation and partial nephrectomy. Cryoablation does have a slightly higher rate of local recurrence (5 to 10 percent versus 1 to 3 percent), but recurrences are caught early on surveillance imaging and retreated with a second ablation, and cancer-specific survival remains equivalent.
Technical success — meaning complete tumor destruction confirmed on imaging — is achieved in 94 to 100 percent of cases for T1a tumors. For tumors under three centimeters, success rates reach 97 to 100 percent. Disease-specific survival is 94 percent at both five and ten years. Metastasis-free survival is 94.4 percent at five years and 91 percent at fifteen years.
The destroyed tumor tissue remains in place initially, but it is no longer alive. The freezing process kills every cell within the treatment zone. Over the following months, your immune system gradually absorbs the dead tissue, and the area shrinks — approximately 26 percent at three months, 56 percent at one year, and 75 percent at three years. It eventually resolves into a small scar or area of fat. Follow-up imaging confirms there is no living tumor remaining.
Remarkably mild. Studies report average pain scores of just 1.8 out of 10 on the first day. Freezing has a natural anesthetic effect on nerve endings, making cryoablation less painful than heat-based ablation techniques. Seventy-two percent of patients achieve 90 to 100 percent pain relief by day ten. Many patients use only over-the-counter acetaminophen during recovery, and some require no pain medication at all. During the procedure itself, you feel nothing — general anesthesia ensures you are completely asleep.
Most patients go home the same day and return to light activities within two to three days. Full recovery to baseline typically takes one to two weeks. Compare this to partial nephrectomy: three-to-five-day hospital stay and four to six weeks of restricted activity. The hospital stay alone is nearly two days shorter with cryoablation on average.
One of cryoablation's greatest advantages is superior kidney function preservation. Because only the tumor and a small margin are destroyed — not a section of kidney surgically removed — the impact on overall kidney function is minimal. At three years, 95 percent of cryoablation patients remain free of chronic kidney disease, compared to just 70 percent after partial nephrectomy. This is especially important for patients with diabetes, hypertension, or a single functioning kidney.
Ideal candidates are tumors four centimeters or smaller (stage T1a). Tumors three centimeters or smaller achieve the highest success rates of 97 to 100 percent. Tumors in the three-to-four centimeter range are also very treatable with excellent results, typically using additional cryoprobes. Tumors larger than four centimeters may be treatable in select cases but generally achieve better outcomes with surgical removal.
Local recurrence occurs in approximately 5 to 10 percent of cases. However, the structured surveillance program — with imaging at one, three, six, and twelve months, then annually — catches any recurrence early, typically when it is small and easily retreatable with a second cryoablation session. Cancer-specific survival is equivalent to surgery even accounting for this retreatment rate. Metastasis-free survival is 94.4 percent at five years and 91 percent at fifteen years.
Yes. Kidney cryoablation (CPT code 50593) is covered by virtually all major insurance plans when medically indicated, including Blue Cross Blue Shield of Alabama, Medicare, TRICARE, UnitedHealthcare, Aetna, and Cigna. Prior authorization is required, and our team manages this process for you. Medicare hospital outpatient reimbursement is approximately $10,400 for the facility fee. Your out-of-pocket cost depends on your specific plan.
If you have a small kidney tumor (four centimeters or smaller) and were told surgery is your only option without any mention of cryoablation or thermal ablation, seeking a second opinion from an interventional radiologist is reasonable. The American Urological Association, NCCN, and European Association of Urology all endorse thermal ablation as an appropriate treatment for T1a kidney masses. Not all urologists routinely discuss ablation options, and an interventional radiology consultation ensures you understand all guideline-supported treatments before making a decision.
An interventional radiologist is a physician who completes medical school, a radiology residency, and an additional fellowship specifically in image-guided, minimally invasive procedures. Their unique expertise is using advanced imaging (CT, ultrasound, fluoroscopy) to guide instruments precisely to targets inside the body through tiny skin punctures — without surgical incisions. Kidney cryoablation is performed by an interventional radiologist because the procedure depends entirely on real-time image guidance to place probes accurately within the tumor and monitor the ice ball formation. This is a core competency of interventional radiology training.
Yes. One of cryoablation's key advantages is its repeatability. Because it preserves healthy kidney tissue rather than removing it, the procedure can be performed multiple times — whether for retreatment of residual tumor at the original site, a new tumor in the same kidney, or a tumor in the opposite kidney. This is particularly valuable for patients with hereditary syndromes who may develop multiple tumors over their lifetime.
Approximately 20 to 30 percent of small kidney masses are benign. A biopsy is typically performed at the beginning of the cryoablation procedure to determine the diagnosis. Even if the mass is benign, many patients and physicians choose to proceed with ablation to eliminate the need for years of surveillance imaging and the anxiety of monitoring an indeterminate lesion. Treating a benign mass with cryoablation carries very low risk and provides definitive resolution.
Most kidney cryoablations are performed under general anesthesia, meaning you are completely asleep and feel nothing. In select cases, the procedure can be performed under conscious sedation — where you are deeply relaxed but not fully unconscious. Dr. Bourgeois and the anesthesia team determine the best approach based on your health, the tumor location, and your comfort preferences.
Cryoablation (freezing) and radiofrequency ablation (heating) are both image-guided ablation techniques, but cryoablation has emerged as the preferred method for kidney tumors. Comparative studies show cryoablation has fewer retreatments (1.3 percent versus 8.5 percent), lower tumor progression rates (5.2 percent versus 12.9 percent), a visible treatment zone on CT for real-time monitoring, less procedural pain, and greater safety near the collecting system and ureter. These advantages explain why cryoablation is the dominant kidney ablation technique at major academic centers.
Have more questions? Dr. Bourgeois is happy to discuss your specific situation.
Schedule Your Consultation