")
Liver Microwave Ablation
Destroy Small Liver Tumors with Precision Heat — Without Surgery
Home » Liver Microwave Ablation
A Potentially Curative Treatment for Small Liver Tumors
When liver tumors are small enough to be destroyed completely, microwave ablation offers something most liver cancer treatments cannot: a realistic chance at cure — without a single surgical incision.
Microwave ablation uses a thin, needle-like probe inserted through the skin directly into the tumor. When activated, the probe generates intense, precisely targeted heat that destroys cancer cells in minutes. The destroyed tissue is gradually replaced by harmless scar tissue that shrinks over time. For small liver tumors under three centimeters, clinical studies show that microwave ablation achieves survival outcomes comparable to surgical removal — with dramatically less pain, shorter recovery, and fewer complications.
This is not a new or experimental treatment. Thermal ablation has been recommended by every major cancer guideline organization for over a decade, and microwave technology represents the latest and most powerful generation — creating larger treatment zones faster and more reliably than the older radiofrequency approach it has largely replaced.
The procedure typically takes one to three hours, most patients go home the next morning, and the majority return to their normal routine within one to two weeks. Compare that to liver surgery, which typically requires a week-long hospital stay and four to eight weeks of recovery.
Dr. Austin Bourgeois performs liver microwave ablation along with chemoembolization (TACE) and Y90 radioembolization — giving him the expertise to recommend whichever liver-directed therapy offers the best outcome for your specific situation. For patients with small, early-stage tumors, ablation is often the most powerful option available.
Hepatocellular Carcinoma (HCC)
Primary liver cancer is the most common reason for liver microwave ablation. For early-stage HCC — particularly tumors under three centimeters — international guidelines recommend ablation as a first-line curative treatment alongside surgery. In patients who are not surgical candidates due to cirrhosis, tumor location, or overall health, microwave ablation achieves comparable long-term survival with significantly less risk. Complete tumor destruction rates exceed 95% for small tumors.
Colorectal Cancer Liver Metastases
When colon or rectal cancer spreads to the liver, microwave ablation can destroy isolated metastatic tumors that cannot be surgically removed or when surgery would require removing too much healthy liver tissue. Studies show local tumor control rates above 90% with modern microwave technology, and ablation can be repeated if new metastases appear — preserving liver volume for future treatments. Ablation is frequently combined with systemic chemotherapy as part of a comprehensive treatment plan.
Intrahepatic Cholangiocarcinoma
Small bile duct cancers within the liver that are not amenable to surgical resection may be candidates for microwave ablation. A multicenter study published in The Lancet showed comparable survival outcomes between ablation and surgery for cholangiocarcinoma tumors within Milan criteria, making ablation a viable curative-intent option for select patients with this challenging diagnosis.
Neuroendocrine Tumor Liver Metastases
Carcinoid tumors and other neuroendocrine tumors that have spread to the liver respond well to thermal ablation, particularly when there are a limited number of well-defined lesions. Ablation can provide effective symptom relief from hormonal syndromes while controlling tumor growth. Its repeatability makes it especially valuable for neuroendocrine patients, who often experience slow-growing recurrent disease over years.
Bridge to Liver Transplant
For patients awaiting liver transplant, microwave ablation can control tumor growth during the waiting period and prevent progression that would disqualify them from transplantation. Ablation can also downstage tumors — shrinking them enough to meet transplant eligibility criteria when they initially exceeded size limits.
Tumors in Challenging Locations
Microwave ablation is particularly effective for tumors near major blood vessels where older radiofrequency technology struggled. The microwave energy overcomes the cooling effect of nearby blood flow — known as the heat-sink effect — that historically caused incomplete treatment and higher recurrence rates with radiofrequency ablation.
HOW MICROWAVE ABLATION WORKS
Microwave ablation works on the same principle as a microwave oven — but with far greater precision and power, focused on an area smaller than a golf ball.
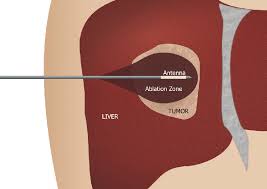
A thin antenna, roughly the diameter of a coffee stirrer, is guided through the skin and into the center of the liver tumor using real-time CT or ultrasound imaging. Once positioned, the antenna emits electromagnetic waves at a specific frequency that causes water molecules inside the tumor cells to vibrate rapidly — millions of times per second. This molecular friction generates intense heat, rapidly raising the temperature inside the tumor above 60 degrees Celsius (140 degrees Fahrenheit). At these temperatures, cancer cells are destroyed almost instantly through a process called coagulative necrosis.
The treatment zone is intentionally created five to ten millimeters larger than the visible tumor in all directions. This safety margin — called the ablation margin — ensures that microscopic cancer cells surrounding the tumor are also destroyed. Research shows that achieving an adequate margin is the single most important factor in preventing the cancer from returning at the treatment site.
The entire ablation process for a single tumor takes roughly two to ten minutes of active energy delivery. Once the tumor is destroyed, the antenna is slowly withdrawn while cauterizing the insertion track to prevent bleeding and the extremely rare possibility of tumor cell seeding along the needle path.
Over the following weeks and months, your body’s immune system gradually absorbs the destroyed tissue. On follow-up imaging, the treated area appears as a shrinking area of scar tissue — with no living cancer cells remaining if the ablation was successful.
Why Microwave Instead of Radiofrequency?
If you have researched liver ablation, you may have encountered references to radiofrequency ablation (RFA) — the older thermal ablation technology that has been used since the 1990s. While RFA was a breakthrough in its time, microwave ablation has largely replaced it at most major cancer centers due to several important advantages:
Microwave ablation reaches higher temperatures faster — creating effective treatment zones in two to ten minutes compared to twelve to twenty minutes or more with radiofrequency. It creates larger, more predictable ablation zones, which improves the chances of achieving complete tumor destruction with adequate safety margins. Most importantly, microwave energy is significantly less affected by the heat-sink effect — the tendency for nearby blood vessels to cool the treatment zone and leave cancer cells alive. Clinical studies show that switching from radiofrequency to microwave technology reduces the risk of incomplete treatment by 30 to 45 percent.
Microwave ablation also eliminates the need for grounding pads that radiofrequency requires, removing the small but real risk of skin burns at pad sites. And unlike radiofrequency, microwave systems can operate multiple antennas simultaneously to treat several tumors at once or create larger treatment zones for bigger tumors.
Dr. Bourgeois uses the latest-generation microwave ablation technology to give patients the best possible chance of complete tumor destruction with a single treatment session


Who is a Candidate?
Is Liver Microwave Ablation Right for You?
The best candidates for liver microwave ablation typically have tumors three centimeters or smaller (up to five centimeters with technique modifications), no more than five to six. During your consultation, Dr. Bourgeois reviews your imaging, lab work, and medical history to determine whether microwave ablation, chemoembolization, Y90 radioembolization, or a combination approach offers the best outcome for your specific situation.
Small Liver Tumors That Cannot Be Surgically Removed
The most common scenario: you have been diagnosed with one or more liver tumors under three to five centimeters, but surgery is not recommended — either because of underlying cirrhosis, tumor location near critical blood vessels, insufficient remaining healthy liver, or overall health factors that make a major operation too risky. For these patients, microwave ablation provides a curative-intent treatment with outcomes that rival surgery for small tumors.
Patients Who Prefer a Less Invasive Alternative to Surgery
Even when surgery is technically possible, some patients and their physicians choose ablation for tumors under three centimeters because it achieves comparable survival with dramatically less impact on the body. Hospital stays are measured in hours rather than days. Recovery is measured in weeks rather than months. And because ablation preserves more healthy liver tissue, it keeps more treatment options available if new tumors develop in the future.
Patients with Multiple Small Tumors
Microwave ablation can treat multiple tumors — up to five or six — in a single session using multiple antennas simultaneously. This is particularly valuable for patients with several small metastatic tumors scattered through the liver, where surgery would require removing too much healthy tissue.
Patients Needing Tumor Control Before or After Other Treatments
Ablation works effectively in combination with other therapies. It can be combined with chemoembolization (TACE) for tumors in the three-to-five centimeter range — where TACE first reduces blood flow to the tumor, then ablation delivers the killing blow. It can also be performed before or after systemic chemotherapy, and can serve as a bridge therapy for patients awaiting liver transplant.
What to Expect: Your Microwave Ablation Journey
Consultation and Treatment Planning
Dr. Bourgeois reviews your diagnosis, imaging studies, lab results, and complete medical history. He explains how microwave ablation works, discusses whether your tumor size, number, and location make you a strong candidate, and compares ablation to other treatment options. If you have been referred by an oncologist, hepatologist, or surgeon, he coordinates directly with your care team to align on the treatment plan. Pre-procedure blood work — including liver function, kidney function, coagulation studies, and tumor markers — is obtained. You receive specific instructions about stopping blood thinners (typically five to seven days for aspirin, three to seven days for prescription anticoagulants), fasting requirements, and what to expect on procedure day.
Procedure Day
You arrive at the hospital and check in at the day surgery unit. An IV is placed, monitoring equipment is attached, and you change into a hospital gown. For most liver ablations, general anesthesia is used — you will be completely asleep and feel nothing during the procedure. Once you are under anesthesia, the interventional radiology team positions you in the CT scanner. Using CT imaging for precise guidance, Dr. Bourgeois makes a small skin puncture — just a few millimeters — and advances the thin microwave antenna through the liver tissue into the center of the tumor.
A contrast-enhanced scan confirms exact positioning. The microwave generator is then activated, delivering targeted energy for two to ten minutes per tumor. You may hear a gentle humming sound from the generator, though under general anesthesia you will not be aware of it. After ablation is complete, a verification CT scan is performed immediately — while you are still under anesthesia — to confirm the entire tumor has been treated with adequate margins. If any area appears undertreated, additional ablation is performed during the same session. The antenna is withdrawn while cauterizing the insertion track, and a small bandage is applied. No stitches are needed. The entire procedure typically takes one to three hours, though the actual ablation time per tumor is usually under ten minutes.
Recovery and Discharge
Most patients go home the same day and return to work within three to seven days. You may experience mild pelvic discomfort and increased urinary frequency during the first few days — this is temporary and indicates the procedure is working.
You wake up in the recovery area and are monitored for several hours. Vital signs, pain levels, and the skin puncture site are checked regularly. Most patients experience mild soreness at the insertion site and some general fatigue. Pain medication is available but many patients require only over-the-counter options. Blood work is drawn to check liver function. Once you are eating, drinking, and comfortable with oral medication, you are cleared for discharge. Most patients go home the morning after the procedure, and some same-day discharges are possible for straightforward cases.
Recovery at Home and Follow-Up
You go home with instructions to rest for the first few days, keep the puncture site clean and dry, and avoid heavy lifting for one to two weeks. Most patients feel noticeably better each day and return to light activities and desk work within one week. Full recovery to baseline energy levels typically takes two to three weeks — a fraction of the four-to-eight-week recovery after liver surgery. Your first follow-up imaging scan — a contrast-enhanced CT or MRI — is performed at approximately one month to confirm complete tumor destruction and establish a baseline for future comparison. After that, imaging is repeated every three months for the first year, then every three to six months ongoing, to monitor for any new tumor development.
How Many Treatments Will I Need?
Many patients require only a single ablation session. Additional sessions may be needed if you have multiple tumors that are treated in stages, if follow-up imaging reveals an area of incomplete treatment that needs retreatment, or if new tumors develop months or years later. One of the key advantages of ablation over surgery is its repeatability — the procedure can be performed multiple times because it preserves healthy liver tissue rather than removing it.
Why Patients Choose Microwave Ablation






Ablation vs. Other Liver Cancer Treatments
Choosing the right liver cancer treatment depends on tumor size, number, location, liver function, and overall health. Here is how microwave ablation compares to other common approaches — and how Dr. Bourgeois helps you navigate the decision:
Microwave Ablation vs. Surgical Resection
- For tumors under three centimeters, multiple studies show no significant difference in long-term survival between ablation and surgery. The survival gap only emerges for larger tumors (three to five centimeters) and at longer time horizons (seven-plus years).
- Ablation has dramatically shorter recovery: one to two weeks versus four to eight weeks for surgery. Hospital stay is typically one night versus five to seven nights.
- Major complication rates are significantly lower with ablation (3 to 5 percent versus 17 percent). Blood loss averages 50 milliliters versus 200 or more.
- Surgery removes an entire section of liver; ablation preserves healthy tissue. This matters for patients with limited liver function or who may need future treatments.
- Surgery remains preferred for larger tumors (greater than three centimeters) and when complete surgical removal with clear margins is achievable.
Microwave Ablation vs. Chemoembolization (TACE)
These are complementary treatments that work best for different tumor sizes:
- Ablation is the preferred approach for small tumors (under three centimeters) because it can achieve complete destruction — a potentially curative outcome. TACE is the preferred approach for larger or more numerous tumors where complete destruction with ablation alone is not feasible.
- For tumors in the three-to-five centimeter range, ablation and TACE are often combined: TACE first reduces blood flow to the tumor, then ablation delivers the final treatment. This combination achieves complete tumor response in 65 percent of cases, compared to 38 percent with TACE alone.
- Ablation is typically a single outpatient procedure. TACE usually requires an overnight hospital stay and averages two to three sessions.
- Bourgeois performs both procedures and selects or combines them based on your specific tumor characteristics.
- Internal link: Learn more about Chemoembolization (TACE) → /chemoembolization-tace-huntsville
Microwave Ablation vs. Y90 Radioembolization
- Ablation uses heat to destroy tumors directly; Y90 delivers targeted radiation through microscopic beads injected into the tumor blood supply. Both are minimally invasive and performed by an interventional radiologist.
- Ablation is preferred for small, well-defined tumors where complete destruction is the goal. Y90 is preferred for larger tumors, diffuse disease, or tumors with portal vein invasion — situations where ablation cannot safely cover the entire tumor.
- Ablation offers the fastest recovery of all liver-directed therapies (one to two weeks). Y90 is also well-tolerated but fatigue can persist for several weeks.
- Both treatments preserve healthy liver tissue and can be repeated. Dr. Bourgeois performs both and recommends the approach best suited to your tumor characteristics.
- Internal link: Learn more about Y90 Radioembolization → /y90-radioembolization-huntsville
Your Recovery Timeline After Liver Microwave Ablation
One of the most common things we hear from patients after liver ablation is that recovery was easier than they expected. That said, we believe in preparing you honestly so there are no surprises.
Understanding the Investment in Your Treatment
We believe in financial transparency because worrying about costs should not add to the stress of a cancer diagnosis.
Liver microwave ablation is one of the most cost-effective liver cancer treatments available. A national SEER-Medicare analysis found that the median total cost for percutaneous ablation is approximately $6,700 — compared to roughly $25,600 for surgical resection and $66,000 for liver transplant. For patients with Medicare, median out-of-pocket costs are approximately $1,200 for the procedure itself, rising to around $2,100 when including follow-up care through 90 days.
Microwave ablation is broadly covered by insurance when medically indicated. Blue Cross Blue Shield of Alabama, Medicare, Medicaid, TRICARE, UnitedHealthcare, Aetna, and Cigna all cover liver ablation for standard indications including hepatocellular carcinoma and colorectal liver metastases in appropriate candidates. Prior authorization is typically required, and our team handles this process on your behalf.
For Medicare patients, Part B covers 80 percent of the approved amount after your annual deductible. Medigap supplemental plans often cover the remaining 20 percent coinsurance.
Veterans receiving care through the VA system may be eligible for community care authorization to receive liver ablation locally in Huntsville rather than traveling to the Birmingham VA Medical Center. Our office can assist with the referral and authorization process for VA patients.
Before your procedure, our team verifies your insurance coverage, obtains necessary authorizations, and provides you with a clear estimate of expected out-of-pocket costs so you can plan accordingly.



What If My Tumor Is Too Large for Ablation Alone?
Not every liver tumor is best treated with ablation alone — and we believe in being upfront about that from the start. Here is how Dr. Bourgeois approaches tumors that fall outside the ideal ablation window, and what options exist when ablation is part of a multi-treatment strategy:
Combined TACE Plus Ablation for Larger Tumors: For tumors in the three-to-five centimeter range, chemoembolization (TACE) and microwave ablation are often performed together. TACE is delivered first to cut off the tumor blood supply, which eliminates the heat-sink effect and allows the subsequent ablation to be more effective. Studies show this combination achieves complete tumor response in 65 percent of patients — nearly double the rate of TACE alone — with significantly longer time before local tumor progression.
Y90 Radioembolization for Diffuse or Large Tumors: When tumors are too large, too numerous, or too diffuse for ablation, Y90 radioembolization delivers targeted radiation through microscopic beads to the tumor blood supply. Dr. Bourgeois performs both procedures and can transition seamlessly between them based on your tumor response.
Systemic Therapy Integration: Microwave ablation works effectively alongside systemic chemotherapy, immunotherapy, and targeted therapy. Your oncologist may recommend ablation to eliminate visible liver tumors while systemic treatment addresses microscopic disease elsewhere. Ablation does not interfere with most systemic regimens and the rapid recovery allows patients to resume their other treatments quickly.
Liver Transplant Pathway: For patients whose liver function is severely compromised by cirrhosis, ablation may serve as a bridge to transplant — controlling tumors while you await a donor organ. Ablation can also downstage tumors that initially exceed transplant size criteria, potentially qualifying you for a curative transplant.
Surveillance After Successful Ablation: If your ablation achieves complete tumor destruction confirmed on imaging, you enter an active surveillance program with imaging every three months. While new tumors can develop — particularly in patients with underlying cirrhosis or ongoing hepatitis — catching them early through regular monitoring means they can often be treated with repeat ablation before they grow large enough to require more intensive therapies.
The key advantage: Dr. Bourgeois offers microwave ablation, chemoembolization, and Y90 radioembolization — the full spectrum of liver-directed therapies performed by an interventional radiologist. This means your treatment recommendation is guided by what is best for your tumor, not by what a particular facility happens to offer.

Expert Liver Tumor Treatment — Close to Home
Dr. Austin Bourgeois brings academic medical center-caliber liver tumor treatment to Huntsville. His credentials include:
- Board-certified in both Diagnostic Radiology and Interventional Radiology & Diagnostic Radiology
- Fellowship-trained in Vascular and Interventional Radiology at the Medical University of South Carolina — one of the nation’s premier IR training programs — with specialized training in interventional oncology and thermal ablation
- Published researcher in interventional oncology with peer-reviewed manuscripts on liver-directed therapy techniques and outcomes in the Journal of Vascular and Interventional Radiology (JVIR)
- Member of the JVIR editorial board
- Performs the full spectrum of liver-directed therapies: microwave ablation, chemoembolization (TACE), and Y90 radioembolization — allowing truly unbiased treatment recommendations based on what works best for each patient
- Boston Scientific TheraSphere Advanced User, indicating proctor-level expertise in liver-directed therapies
- Practicing in North Alabama since 2016 with established relationships across the regional oncology, gastroenterology, and hepatology referral network
What this means for you: your liver ablation is performed by a physician with published research in the field, editorial-board-level involvement in the specialty’s leading journal, and the procedural expertise that comes from offering not just one but all three liver-directed therapies. You receive the same quality of care available at major academic cancer centers — with the convenience of staying in Huntsville, close to your family, your oncologist, and your support system.
Whether you have been referred by Clearview Cancer Institute, your gastroenterologist, your hepatologist, or are seeking a second opinion on a treatment plan, Dr. Bourgeois welcomes the opportunity to review your case and discuss your options.
Frequently Asked Questions
Quick answers about liver microwave ablation — what to expect, recovery, and results.
For small hepatocellular carcinoma tumors under two to three centimeters, microwave ablation is considered a potentially curative treatment. Multiple clinical studies show no significant difference in long-term survival between ablation and surgical removal for tumors in this size range. This is a procedure performed with curative intent — not just disease control. Success depends on tumor size, achieving adequate treatment margins, and the underlying liver condition.
Technical success — meaning complete tumor destruction confirmed on imaging — is achieved in 95 to 99 percent of tumors under three centimeters. A major 2025 real-world registry study of over 600 patients across 24 medical centers reported 98 percent technical success and 12-month overall survival of 96 percent. For tumors under one centimeter, local recurrence rates are under 7 percent at two years.
Microwave ablation is the newer, more powerful technology that has largely replaced radiofrequency at most major cancer centers. It reaches higher temperatures faster, creates larger and more predictable treatment zones, and is significantly less affected by blood flow cooling near vessels. Clinical studies show microwave reduces the risk of incomplete treatment by 30 to 45 percent compared to radiofrequency. It also treats tumors faster — typically two to ten minutes versus twelve to twenty minutes per tumor.
During the procedure itself, you feel nothing — most liver ablations are performed under general anesthesia. After the procedure, pain is typically mild, averaging three to four out of ten on a pain scale. Most patients manage with over-the-counter pain relief. Some patients experience referred pain in the right shoulder for one to three days due to diaphragm irritation — this is common and resolves on its own. We proactively manage pain so you are never asked to tough it out.
Most patients go home the day after the procedure and return to light activities and desk work within one week. Full recovery to baseline energy levels typically takes two to three weeks. Compare this to liver surgery, which requires a five-to-seven-day hospital stay and four to eight weeks of recovery. Some patients with very small tumors treated percutaneously may be discharged the same day.
Approximately one in four patients develops low-grade fever, fatigue, body aches, and mild nausea beginning three to five days after the procedure and lasting five to ten days. This is not a complication — it is your immune system responding to the destroyed tumor tissue being broken down and absorbed. It is actually a sign that the treatment worked. Symptoms are managed with over-the-counter acetaminophen. If you do not experience it, that is equally normal.
Ideal candidates are tumors three centimeters or smaller, where complete ablation rates exceed 95 percent and outcomes rival surgery. Tumors up to five centimeters can be treated with technique modifications such as multiple antenna placements or combination with chemoembolization. For tumors larger than five centimeters, other liver-directed therapies such as TACE or Y90 radioembolization are generally more appropriate. Dr. Bourgeois offers all three and recommends the best fit for your specific tumor.
Yes. Liver ablation is covered by virtually all major insurance plans when medically indicated, including Blue Cross Blue Shield of Alabama, Medicare, TRICARE, UnitedHealthcare, Aetna, and Cigna. Prior authorization is required, and our team manages this process for you. A national cost analysis found liver ablation to be the most cost-effective liver cancer treatment available, with Medicare out-of-pocket costs averaging approximately twelve hundred dollars for the procedure.
Yes. Microwave ablation can treat multiple tumors in a single session — up to five or six tumors depending on their size and location. Modern microwave systems can operate multiple antennas simultaneously, allowing treatment of several tumors at once. This is particularly valuable for patients with multiple small metastatic tumors.
Many patients need only a single session. Additional treatments may be necessary if you have multiple tumors treated in stages, if follow-up imaging reveals a small area of incomplete treatment that needs retreatment, or if new tumors develop months or years later. One of ablation's key advantages is its repeatability — because it preserves healthy liver tissue, it can be performed multiple times without compromising liver function.
The destroyed tumor cells become inert scar tissue. Your immune system gradually absorbs this tissue over the following weeks and months. On follow-up imaging, the treated area appears as a shrinking area of scar with no blood flow — confirming that no living cancer cells remain. The ablation zone is intentionally larger than the original tumor because of the safety margin included during treatment.
Ablation may not be appropriate for patients with tumors larger than five centimeters (unless combined with TACE), tumors in certain locations directly adjacent to the bile ducts, gallbladder, stomach, or bowel where heat could cause injury, severely compromised liver function (Child-Pugh class C), cancer that has spread extensively outside the liver, active untreated infection, or significant blood clotting disorders. These factors are carefully evaluated during your consultation.
Have more questions? Dr. Bourgeois is happy to discuss your specific situation.
Schedule Your Consultation