")
Pelvic Congestion Embolization
Finally, an Answer to Years of Chronic Pelvic Pain
Home » Pelvic Congestion Embolization
If you’ve spent years dealing with unexplained pelvic pain — pain that worsens when you stand or sit for too long, improves when you lie down, and disrupts your daily life — you’re not alone, and you’re not imagining it.
Pelvic congestion syndrome (PCS) affects thousands of women in North Alabama, yet it often goes undiagnosed for an average of 6 to 7 years while patients are told their pain is “normal,” psychosomatic, or misattributed to endometriosis or IBS. Up to 30 percent of all chronic pelvic pain cases are caused by pelvic congestion syndrome.
Dr. Austin Bourgeois is the only interventional radiologist in Huntsville offering pelvic vein embolization — a proven, minimally invasive treatment that addresses the root cause of your pain. Women in North Alabama no longer need to travel 100+ miles to Birmingham or Nashville for relief. With a 98 to 100 percent technical success rate and 85 to 95 percent symptom improvement, embolization delivers lasting results with same-day discharge, no surgery, and a 1 to 2 day recovery. No referral is needed to schedule a consultation.
BENEFITS OF PELVIC VEIN EMBOLIZATION
- No surgical incision — just a tiny needle puncture
- No general anesthesia or breathing tube required
- Same-day discharge with no overnight hospital stay
- Preserves the uterus, ovaries, and fertility — safe for future pregnancy
- Return to work in 1-2 days vs. 6+ weeks for hysterectomy
- Low complication rate (~9%) with zero reported deaths in published literature
- Treats multiple veins (ovarian and internal iliac) in one session
- Equivalent or superior results to hysterectomy with dramatically faster recovery
- Diagnosis and treatment in a single visit via catheter venography
Is Pelvic Congestion Syndrome Affecting Your Life?
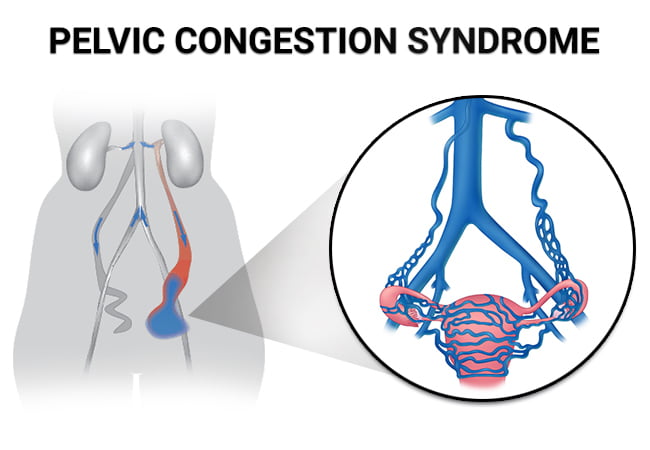
Pelvic congestion syndrome occurs when veins in the pelvis develop faulty valves, allowing blood to pool — similar to varicose veins in the legs, but inside the pelvis where they are invisible and much harder to diagnose. Common symptoms include:
- Chronic dull, aching pelvic pain lasting 6+ months that worsens with standing or sitting
- Pain that improves when lying down — the hallmark symptom of PCS
- Deep pain during or after intercourse (dyspareunia)
- Painful or heavy menstrual periods
- Visible varicose veins on the vulva, inner thighs, or buttocks
- Pelvic pressure or heaviness that worsens throughout the day
- Lower back pain
- Urinary urgency or frequency
PCS most commonly affects women of childbearing age, especially after pregnancy. If you’ve been treated for endometriosis, IBS, or musculoskeletal pain without finding relief, pelvic congestion syndrome may be the underlying cause that was never identified.
WHAT IS PELVIC CONGESTION EMBOLIZATION?
Pelvic vein embolization (also called ovarian vein embolization) treats pelvic congestion syndrome without surgery. Dr. Bourgeois guides a thin catheter through a tiny needle puncture in the groin or neck to the faulty pelvic veins using real-time X-ray imaging. Tiny metallic coils and a medical foam agent are placed to seal these veins, redirecting blood flow through healthy pathways and eliminating the source of pain.
The procedure takes 60 to 90 minutes under conscious sedation — no general anesthesia, no surgical incision, and you go home the same day. Diagnostic venography is performed at the start of the procedure, meaning diagnosis and treatment happen in a single visit. Dr. Bourgeois can treat multiple veins (ovarian and internal iliac tributaries) in one session.
In the only randomized controlled trial comparing treatments, embolization reduced pain more effectively than hysterectomy — while preserving fertility and avoiding major surgery.


Who is a Candidate for Pelvic Congestion Embolization
Chronic Pelvic Pain
Chronic pelvic pain lasting 6+ months that worsens with standing, sitting, or at the end of the day and improves when lying down
Intense Pain
Deep pain during or after intercourse, painful periods, or visible varicose veins on the vulva, inner thighs, or buttocks
Wishing to Preserve Fertility
Women who want to preserve fertility and avoid hysterectomy or other major surgery
Misdiagnosis
Patients misdiagnosed with endometriosis, IBS, or other conditions without finding relief from treatment
Those with a Need for Fast Recovery
Military spouses and active-duty personnel at Redstone Arsenal who need rapid return to activity without extended surgical recovery
What to Expect During Pelvic Vein Embolization
Before the Procedure
You’ll meet with Dr. Bourgeois to review your symptoms, medical history, and imaging studies. Transvaginal ultrasound with Doppler, MRI, or CT venography may be ordered if not already completed. Pre-procedure instructions include fasting for 12 hours and arranging a driver to take you home. You’ll receive detailed preparation guidelines at your consultation.
During the Procedure
After arriving at the outpatient interventional radiology suite, you’ll receive an IV for fluids and moderate sedation — you’ll be relaxed but awake. A small nick is made in the skin at the groin or neck (no stitches needed), and a thin catheter about 1/8 inch in diameter is guided under live X-ray imaging to the pelvic veins.
Contrast dye is injected to create a detailed map of your pelvic venous anatomy — this diagnostic venography confirms which veins are malfunctioning and allows diagnosis and treatment in the same session. Once identified, tiny metallic coils and/or medical foam are deployed to seal the incompetent veins. A follow-up venogram confirms successful closure. The catheter is removed, a Band-Aid is applied, and you’re taken to a recovery area. Total procedure time: 60 to 90 minutes.
After the Procedure
You’ll rest for 2 to 4 hours in recovery while the sedation wears off, then go home the same day with written discharge instructions. Mild pelvic cramping or discomfort for 2 to 5 days is normal and easily managed with over-the-counter pain medication. You should avoid heavy lifting (over 10 pounds) and vigorous exercise for one week. Most patients feel “back to normal” within 3 to 7 days, with full symptom improvement developing over the following 4 to 12 weeks.
Recovery and Results
Most patients go home within 2 to 4 hours of the procedure with a small bandage at the puncture site. Mild pelvic cramping for 2 to 5 days is common and easily managed with over-the-counter ibuprofen or acetaminophen. You should avoid heavy lifting over 10 pounds and vigorous exercise for one week.
Most women return to light activities and desk work within 1 to 2 days and resume full physical activity including exercise within one week. Sexual activity can typically resume after 1 to 2 weeks. Compare this to 6 or more weeks of recovery after hysterectomy and 2 to 4 weeks after surgical vein ligation.
Symptom improvement develops gradually over 4 to 12 weeks as the sealed veins shrink and blood flow normalizes. Studies tracking patients for up to 5 years show sustained, dramatic pain reduction:
• Pain scores drop from an average of 7.3 out of 10 to less than 1 out of 10 at long-term follow-up
• 85 to 95 percent of women experience significant symptom improvement
• In a study of 300+ patients followed for 5 years, 93.85 percent experienced clinical success
• 92 percent report significant pain improvement
• 96 percent report meaningful improvement in daily functioning, intimacy, and emotional wellbeing
• Recurrence rates range from 5 to 13 percent — comparable to surgical alternatives
A follow-up visit documents your improvement and confirms treatment success.
How Pelvic Vein Embolization Compares to Other Treatments
How Pelvic Vein Embolization Compares to Other Treatments
Side-by-side comparison of your treatment options for pelvic congestion syndrome.
| Feature | Embolization ✦ | Hysterectomy | Hormonal Therapy | Surgical Ligation |
|---|---|---|---|---|
| Anesthesia | Conscious sedation | General | None | General |
| Incision | None (needle puncture) | Abdominal incision | None | 2+ small incisions |
| Hospital stay | Same-day discharge | 1–5 days | Outpatient | Same-day to overnight |
| Return to work | 1–2 days | 6+ weeks | N/A | 2–4 weeks |
| Full recovery | 4–7 days | 6–8 weeks | N/A | 2–4 weeks |
| Symptom improvement | 85–95% | 66–97% | Temporary only | 70–85% |
| Fertility preserved | Yes | No | Yes | Yes |
| Treats root cause | Yes | Yes (removes uterus) | No | Yes |
| Recurrence risk | 5–13% | Low | High (stops with meds) | 10–20% |
| Long-term data | 5+ years | Extensive | N/A | Limited |
✦ Dr. Bourgeois performs pelvic vein embolization in Huntsville — the only local provider of this procedure.

North Alabama’s Only Local Pelvic Congestion Embolization Provider
Dr. Austin Bourgeois is a board-certified, fellowship-trained interventional radiologist who brings specialized expertise in minimally invasive vascular procedures to women suffering from pelvic congestion syndrome. Prior to Dr. Bourgeois offering this service in Huntsville, women in North Alabama had to travel over 100 miles to Birmingham or Nashville for pelvic vein embolization — a significant burden when you’re already dealing with chronic pain.
As a member of the Society of Interventional Radiology and with extensive training in advanced image-guided therapies, Dr. Bourgeois understands that chronic pelvic pain isn’t “just something you have to live with” — it’s a real vascular condition with a proven minimally invasive solution. Whether you’re active-duty military at Redstone Arsenal, part of Huntsville’s aerospace workforce, or simply ready to reclaim your quality of life after years of misdiagnosis, you can now receive this life-changing treatment close to home from a physician who specializes in it.
Frequently Asked Questions
Quick answers about pelvic congestion embolization — what to expect, recovery, and results.
Pelvic congestion syndrome (PCS) occurs when veins in the pelvis develop faulty valves, allowing blood to pool — similar to varicose veins in the legs, but inside the pelvis. This pooling creates chronic pelvic pain, typically a dull, aching pressure that worsens with standing and improves when lying down. PCS most commonly affects women of childbearing age, especially after pregnancy. It's estimated to cause up to 30 percent of chronic pelvic pain cases, yet it often goes undiagnosed for an average of 6 to 7 years.
PCS is diagnosed through a combination of symptom evaluation and specialized imaging. Transvaginal ultrasound with Doppler can detect dilated pelvic veins and abnormal blood flow. MRI or CT venography may also be used to map the pelvic venous anatomy in detail. The definitive diagnosis is made during catheter venography — a diagnostic imaging test that can be performed immediately before treatment in the same session, allowing for diagnosis and treatment in one visit.
Through a tiny needle puncture in the skin at the groin or neck, your interventional radiologist guides a thin catheter to the affected pelvic veins using live X-ray imaging. Contrast dye is injected to visualize the veins, then tiny coils and/or a medical foam are placed to seal the faulty veins — redirecting blood through healthy pathways. The entire procedure takes about 60 to 90 minutes under light sedation, and you go home the same day with just a small bandage. No surgical incision, no stitches, no general anesthesia required.
Most patients return to light activities and desk work within 1 to 2 days and resume full activity including exercise within one week. Mild pelvic cramping for 2 to 5 days is common and easily managed with over-the-counter ibuprofen. Sexual activity can typically resume after 1 to 2 weeks. Full symptom improvement develops gradually over 4 to 12 weeks. Compare this to 6+ weeks of recovery after hysterectomy.
Pelvic vein embolization has a 98 to 100 percent technical success rate and achieves meaningful symptom improvement in 85 to 95 percent of women. In a major study of over 300 patients followed for up to 5 years, 93.85 percent experienced clinical success with pain scores dropping from 7.34 to 0.78 out of 10. In the only randomized controlled trial comparing treatments, embolization reduced pain more effectively than hysterectomy.
No. Ovarian vein embolization preserves the uterus, ovaries, and full reproductive function. Recent studies show no significant changes in reproductive hormones after the procedure, and multiple published case series document successful pregnancies and healthy deliveries following embolization. One study of women with PCS-related infertility found a 66.7 percent pregnancy rate after treatment.
Coverage varies by insurance plan. Many insurers cover the procedure with prior authorization and documentation of failed conservative treatment. Practices report routine insurance approval including BCBS, Aetna, UnitedHealthcare, and TRICARE with appropriate documentation and peer-to-peer physician review. Our practice assists with insurance verification, prior authorization, and appeals. Contact our office to discuss your specific insurance situation.
Have more questions? Dr. Bourgeois is happy to discuss your specific situation.
Schedule Your Consultation